The lining of the uterus changes throughout the menstrual cycle in response to the hormones (oestrogen and progesterone) that is produced by the ovaries. Oestrogen is made before the egg ovulates and progesterone is made after the egg ruptures.
Oestrogen enables the lining to grow and progesterone enables the lining to store glycogen. As and when the fertilized egg comes along, the lining can nourish it and enable it to attach itself to the uterus and thus grow. If fertilization has not happened, then the hormone levels decrease and the lining is eventually shed as a period.
There are times when a woman may not ovulate, oestrogen is produced, progesterone is not produced (as in patients with PCOS, perimenopause women, long term use of drugs like tamoxifen and commonly after menopause). In this case, the lining continues to grow in response to oestrogen but it is not shed as there is no progesterone. It is not shed appropriately and the woman may have irregular bleeding and spotting.
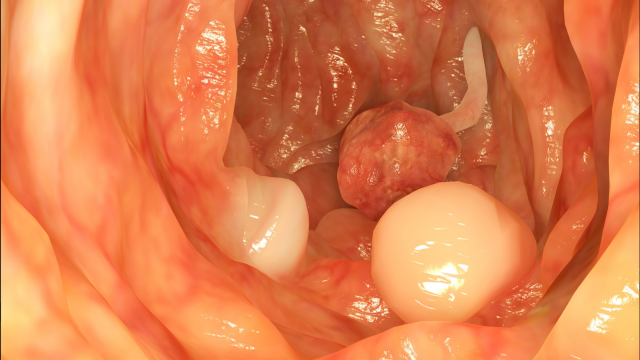
The lining can then become very thick. It is then called hyperplasia. This is not cancer but the same lining can become cancerous in the long run.
Symptoms of Endometrial Hyperplasia
The commonest presenting symptom for endometrial hyperplasia is abnormal bleeding. This may be in form of heavier cycles, longer duration of flow, short cycles, erratic bleeding and bleeding after menopause.
One must report to the gynaecologist in case one as any abnormal bleeding. The doctor will do a complete gynaecological examination and then suggest tests. These may be blood tests and pelvic sonography.
Diagnosis of Endometrial Hyperplasia
The sonography is useful in diagnosing a thick lining. But this is not enough to diagnose hyperplasia.
A definitive diagnosis is obtained only after the doctor takes a small fragment of the lining and it is examined under the microscope to see changes of hyperplasia.
There are various ways of getting a fragment of the lining i.e. endometrial biopsy.
- We can do it in the clinic with a small instrument called endometrial sampler that is easy to insert easily without anaesthesia. It collects a fragment that can then be sent to the histologist for examination.
- The traditional method of Dilatation and curettage is done under anaesthesia and will collect most of the lining.
- The ideal technique is curettage after hysteroscopic visualization of the uterine cavity. This helps the doctor identify and deal with polyps, and helps identify the area in the cavity that looks thickened and abnormal.
Treatment of Endometrial Hyperplasia
Once the diagnosis is confirmed on histology then the treatment can be decided. The treatment will depend on various factors such as:
- Final histology report
- Age of patient.
- Desire for childbearing
The treatment is usually progesterone which can be given as a tablet, singly or in combination with oestrogen, suppository or as an intrauterine device. The doctor will tailor the choice of treatment to suit the needs of the patient.
When there is no remission, recurrence or presence of atypia suggesting a risk of cancer then removal of the uterus is required.
Take an appointment with Dr. Sangeeta, if you think you have any of the above symptoms.