What is Endometriosis?
The lining of the uterus is called endometrium. This tissue grows outside the uterus and then it leads to endometriosis.
The Common Sites
The common sites are the ovaries, the fallopian tubes the part of the pelvis behind the uterus (commonly called pouch of Douglas). It can also grow in the vagina, cervix, vulva, bowel, bladder, or rectum. Very rarely, in distant parts of the body such as the umbilicus, the lungs, brain, and skin.
The Pathology
There is no clarity on why the endometrium develops outside the uterus in some women. There are many theories to explain the same.
The most popular theory is that the menstrual blood flows backward through the fallopian tubes into the pelvis. The ovaries, therefore, is the commonest site for endometriosis. Endometriosis runs in families, and therefore there may be a genetic predisposition. There may be an immunological disturbance that triggers endometrium from growing in an abnormal location.
Endometriosis is sometimes found in scars. This happens in the surgical wounds after surgery like caesarean section and hysterectomy. The endometrium gets implanted in these areas due to surgery and then persists, grows and causes problems.
The endometriotic tissue will grow and bleed every cycle just like the normal endometrium in the menstrual cycle. The difference is that this blood does not exit from the body. This leads to severe irritation and inflammation where ever it is. Thus, it leads to severe pain. After inflammation, there is fibrosis and scarring. This leads to the organs adhering to each other and causing more pain and distortion of anatomy.
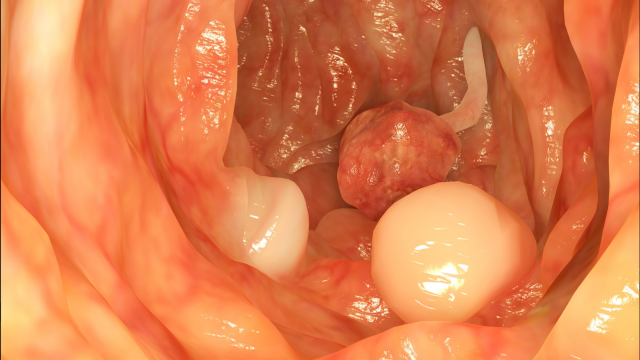
This can be a cause of infertility. The blood on the ovaries can collect in the form of cysts and lead to endometriotic cysts that are commonly called chocolate cysts or endometriomas. Endometriotic tissue usually does not cause cancer.
Endometriosis Symptoms
Pain is the most common symptom. The pain can be varying in duration and intensity. They may have period pains that start even before the period and continue for a few days after the period. They can have pain after sex and after passing the toilet. Some may have chronic pain in the lower back and lower abdomen. Irregular periods or intermenstrual bleeding are also common but can happen due to various pathologies. Patients with Endometriosis also find it difficult to get pregnant and may report for the first time for infertility management.
Endometriosis Diagnosis
The first step is a good detailed history by the doctor. The next step is an internal examination. During an internal examination, it is possible to feel ovarian cysts if present, thickening, and nodules may be felt at the back of uterus which is also suggestive of the endometriosis. Sonography of the pelvis can detect ovarian chocolate cysts if present. In select cases, MRI may be useful.
Laparoscopic examination of the pelvis is the only diagnostic test that can confirm the presence of endometriosis. On laparoscopy, one may see the lesions that are diagnostic, and/or endometriotic cysts, and/or adhesions. On some occasions, a biopsy may be required for histological examination.
Endometriosis Treatment Options
NSAID’s. Pain is a major symptom and needs treatment. NSAID’s are the most effective and can be used where there is no medical contraindication for their use. They are effective in managing pain but will not reduce the lesions. Severe Gastrointestinal irritation is a major side effect that prevents long term use.
Fomentation and acupressure and acupuncture may be tried and may also benefit some.
Birth Control pills: Combined oral contraceptive pills are commonly used and are effective in managing the symptoms and will also heal the lesions to a certain extent. They can be used safely for the long term especially in young women who have no contraindication for their use.
GnRH Agonist: These are injections which are given monthly or every quarterly depending on the dose. They are effective in managing symptoms, reducing the lesions and the size of the cysts. Their side effects are the major limiting factor. They cause estrogen deprivation as a part of their activities and this can lead to hot flashes, vaginal dryness, and decreased libido. The most important side effect is the calcium deprivation from the bone leading to osteoporosis. Therefore, GnRH agonists are generally used for 6 months only.
Progestins: Various progestins have been used, in the management of endometriosis, for eg. Medroxyprogesterone acetate, and norethisterone. Their use is limited mainly due to side effects such as breast pain, weight gain, bloating, and irregular bleeding. The newer generation progestin – Dienogest is a recent addition to the treatment options. It reduces the lesions and the associated pain and can be used effectively for the long term.
Hormonal IUS: This is a great option for women who have undergone surgery and the lesion has been treated and who want contraception. The IUS will not treat lesions and dissolve the cysts but will prevent further Endometriosis lesions from occurring.
Surgery: Surgery is usually chosen for severe symptoms and or as fertility enhancing surgery. It is usually a laparoscopy (Endoscope is inserted into the abdomen and the organs are visualized). The Endometriosis patches can be cauterized, and the adhesions can be cut to free the organs and restore the anatomy as far as possible. Surgery is particularly useful to remove the chocolate cysts. After the surgery, the patient may be given GnRH agonists to suppress the disease or may start with assisted fertility treatments.